Strategies for Delivering LGBT-Inclusive Care

Strategies for Delivering LGBT-Inclusive Care
August 3, 2016 ‐ PSQH
By Jennifer Comerford, MJ, OTR/L, CHC, HEM; and Cynthia Wallace, CPHRM
Discrimination against individuals who identify as lesbian, gay, bisexual, or transgender (LGBT) has been common in many contexts, including healthcare. Consider the following de-identified events reported to the ECRI Institute PSO, a federally certified patient safety organisation (PSO), from January 2013 through mid-2015:
- Physicians made inappropriate comments about an openly gay patient who was intubated.
- A physician abruptly departed from a gay patient’s room after being told about the patient’s positive HIV status.
- Staff refused to modify a transgender patient’s documentation from male to female.
These reports give some indication of discrimination against LGBT individuals. Furthermore, even well-intentioned providers may be genuinely confused about how to ensure that LGBT patients are welcome, understood, and given appropriate access to care.
With the 2015 Supreme Court ruling that same-sex couples have a constitutional right to marry, the anti-discrimination provisions in the Patient Protection and Affordable Care Act of 2010 (PPACA), and the increase in media attention to transgender topics, it is clear that the U.S. is undergoing a sea change regarding legal rights for and social recognition of LGBT individuals.
This awareness is accompanied by a growing acknowledgement that LGBT individuals are at risk for health disparities and being undeserved by healthcare providers, even in the absence of intentional discrimination. For example, LGBT individuals are 2.5 times as likely to have a mental health disorder as heterosexual men and women, and transgender individuals are at increased risk of suicide (Daniel & Butkus, 2015). Of course, discrimination by providers refusing to deliver medical care to LGBT individuals compounds the problem.
Beyond an ethical imperative to provide safe and respectful care to all patients, providers and organisations face a variety of risks—including legal action, loss of federal funding, adverse media attention, citations for failing to adhere to Medicare Conditions of Participation, and accrediting standard violations—for failure to deliver adequate care to LGBT patients. Fortunately, there are a number of steps that providers in ambulatory care and acute care organisations can take to ensure appropriate treatment for all, regardless of sexual orientation or identity.
The diverse individuals of the LGBT community share a “common need for culturally competent health care” that recognises and responds to population-specific medical risks (Health Resources and Services Administration, n.d.). The learning curve to understand these distinctions—and how they can impact a patient’s health status and clinical presentation—may appear steep to providers who do not have expertise addressing gender identity and sexual orientation; however, there are several recommended strategies and many educational resources to help providers deliver LGBT-inclusive care.
The Joint Commission (2011) describes the LGBT population as an “overlooked community” of healthcare consumers disproportionately affected by health disparities. The accrediting agency’s patient-centred communication standards include provisions to prohibit discrimination based on sexual orientation, gender identity, or gender expression. Consistent with Centres for Medicare & Medicaid Services Conditions of Participation, The Joint Commission also requires facilities to protect patients’ rights to choose who may visit them during an inpatient stay regardless of whether the visitor is a family member, same-sex spouse or partner, or other type of visitor.
Section 1557 of PPACA prohibits healthcare providers that receive federal funds from discriminating against patients based on race, national origin, sex, age, or disability. In a final rule published on May 18, 2016, the U.S. Department of Health and Human Services (HHS) definitively established that sex discrimination includes discrimination based on gender identity and sex stereotyping. Although the final rule does not resolve whether discrimination on the basis of an individual’s sexual orientation alone constitutes sex discrimination under Section 1557, HHS states that the agency will continue to follow legal developments in this area and “supports prohibiting sexual orientation discrimination as a matter of policy.” Additionally, the final rule states that the HHS Office for Civil Rights will evaluate allegations of sex discrimination on the basis of an individual’s sexual orientation to determine whether they involve the sorts of stereotyping that can be addressed under Section 1557 (Nondiscrimination in health programs and activities, 2016).
LGBT advocacy groups have also played a major role in setting the agenda for LGBT-inclusive healthcare. For example, the Human Rights Campaign Foundation (2016) publishes data on organisational commitment to LGBT patients and staff in its annual Healthcare Equality Index (HEI) report. To earn leadership status, organisations must have the following core criteria in place:
1.Patient nondiscrimination policies with specific references to sexual orientation and gender identity
2.Equal visitation policies
3.Employment nondiscrimination policies with specific references to sexual orientation and gender identity
4.Staff training in LGBT patient-centred care
Of the 568 facilities completing the 2016 HEI survey, 496 were designated as leaders in LGBT equality, meaning that a minority—fewer than 10%—of approximately 5,900 U.S. hospitals achieved this designation. Survey participation is voluntary and does not reflect the efforts of other healthcare facilities to provide LGBT-inclusive services. The 2016 HEI report compares the results of participating healthcare facilities to findings for more than 900 other “non-respondent” hospitals whose policies were publicly available. Many of these organisations, which represent the majority of U.S. hospitals, fell significantly short in meeting the core criteria for LGBT inclusion (Human Rights Campaign Foundation, 2016).
Health disparities
Research indicates that LGBT individuals experience the following mental and physical health disparities, as well as disparities in access to care:
- Lesbian women are less likely to get preventive cancer screenings. Lesbian and bisexual women are more likely to be overweight or obese (Daniel & Butkus, 2015).
- Gay men are at higher risk of HIV and other sexually transmitted infections (Daniel & Butkus, 2015).
- LGBT individuals have higher rates of smoking, alcohol use, and drug use, and are 2.5 times as likely to have a mental health disorder as heterosexual men and women (Daniel & Butkus, 2015).
- Transgender individuals have a higher lifetime risk for suicide attempts (Daniel & Butkus, 2015).
- LGBT adults and their children are more likely to be uninsured and face difficulties gaining access to care (Daniel & Butkus, 2015).
- LGBT survivors of intimate partner violence face additional challenges, including fear of discrimination, being blamed for the abuse, and involuntary disclosure of sexual orientation (Dunne, 2014).
LGBT individuals also report discrimination when seeking healthcare. In a 2009 survey conducted by Lambda Legal, a civil rights organisation for LGBT persons, about 56% of nearly 5,000 lesbian, gay, or bisexual respondents reported experiencing at least one instance of discrimination (i.e., healthcare professionals refused to provide care, blamed them for their health status, refused to touch them, used harsh or abusive language, or were physically rough or abusive). Rates were higher for transgender and gender-nonconforming respondents and for individuals living with HIV (Lambda Legal, 2010).
More recently, the Human Rights Commission Foundation (2016) reported examples of discrimination including physician’s office staff directing a transgender female patient to a restroom at a nearby fast food restaurant rather than the women’s room in the office’s waiting area, a provider who persisted in calling a transgender man “she” despite his repeated corrections, and an emergency department physician who wanted to do a genital exam on a transgender woman seeking care for a broken rib; when she refused, the physician refused to treat her.
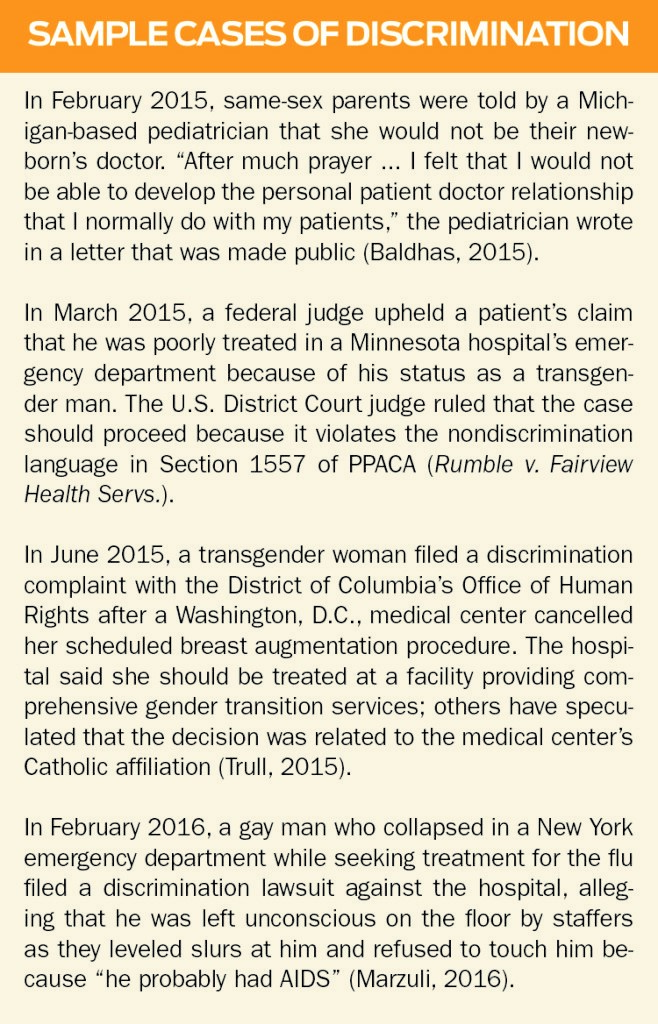
Such discrimination, while often quietly pervasive, is also increasingly being made public; see “Sample Cases” for details. Although high-profile cases in which LGBT patients are refused care may help spark necessary changes in patients’ treatment, they may also make individuals reluctant to seek care in the future, even when life-saving treatment is indicated.
Assessment
Leaders can assess their organisation’s risk exposure in serving the LGBT community by evaluating existing practices. Some have found that the questions posed in the HEI application provide a good framework for inclusion initiatives. The 2016 HEI survey consists of 43 questions about LGBT care practices. Seven of those questions cover the four core criteria that determine HEI leadership status; the rest address best practices for LGBT-inclusive approaches, such as identifying LGBT-knowledgeable providers and designating a contact for LGBT-related matters (see Resource List for the HEI report, an interactive map, and resources for policy development).
Another useful tool to evaluate how well an organisation serves its LGBT population is The Joint Commission’s report, Advancing Effective Communication, Cultural Competence, and Patient- and Family-Centred Care for the Lesbian, Gay, Bisexual, and Transgender (LGBT) Community (2011), commonly referred to as the “field guide” (see Resource List).
Success story
The end result of LGBT-inclusive approaches is not only the delivery of appropriate care, but also improved patient and family satisfaction. For example, in anticipation of the emergency admission of an adolescent transgender female requiring treatment for severe testicular pain, leaders of the Cincinnati Children’s Hospital Medical Centre transgender clinic informed the providers who would be treating the patient of the patient’s transgender status and told them the patient’s preferred name and pronoun. Everyone was prepared by the time the child arrived, and the respectful treatment brought the entire family relief even before surgery (ECRI Institute, 2015).
Strategies
Providers and organisations can take the following steps to increase personal and professional preparedness to treat and serve LGBT patients and families:
- Be mindful of biases. In a study of over 18,000 healthcare providers, researchers found that heterosexual providers had widespread implicit preferences for (e.g., increased comfort with) straight people over lesbian women and, in particular, over gay men. Similarly, lesbian and gay providers held implicit and explicit preferences for lesbian women and gay men over heterosexuals, and bisexual providers held mixed preferences. Researchers called for further investigation as to how implicit sexual prejudice affects care (Sabin, Riskind, & Nosek, 2015).
- Educate providers and support staff about LGBT-inclusive approaches. In addition to increasing knowledge and skills, these experiences are also moderately effective in changing attitudes (Sabin et al., 2015). HEI participants can access training programs at no charge, and the Gay and Lesbian Medical Association (GLMA) provides free access to a four-part webinar series on LGBT healthcare (see Resource List).
- Provide more targeted training as indicated. For example, registration and admission staff should be trained to ask questions about sexual orientation, gender identity, and preferred name and pronoun while respecting the patient’s right to privacy. The Fenway Institute, which provides education and training on LGBT issues, has developed a toolkit for collecting information about sexual orientation and gender identity in clinical settings, including suggestions for how to ask specific questions (see Resource List).
- Employ methods likely to mitigate implicit biases, such as use of clinical guidelines, development of policies to promote objective decision-making, inclusion of counter-stereotypical experiences in educational programs, and eliminating provider discretion from decision-making (Magdali, 2015).
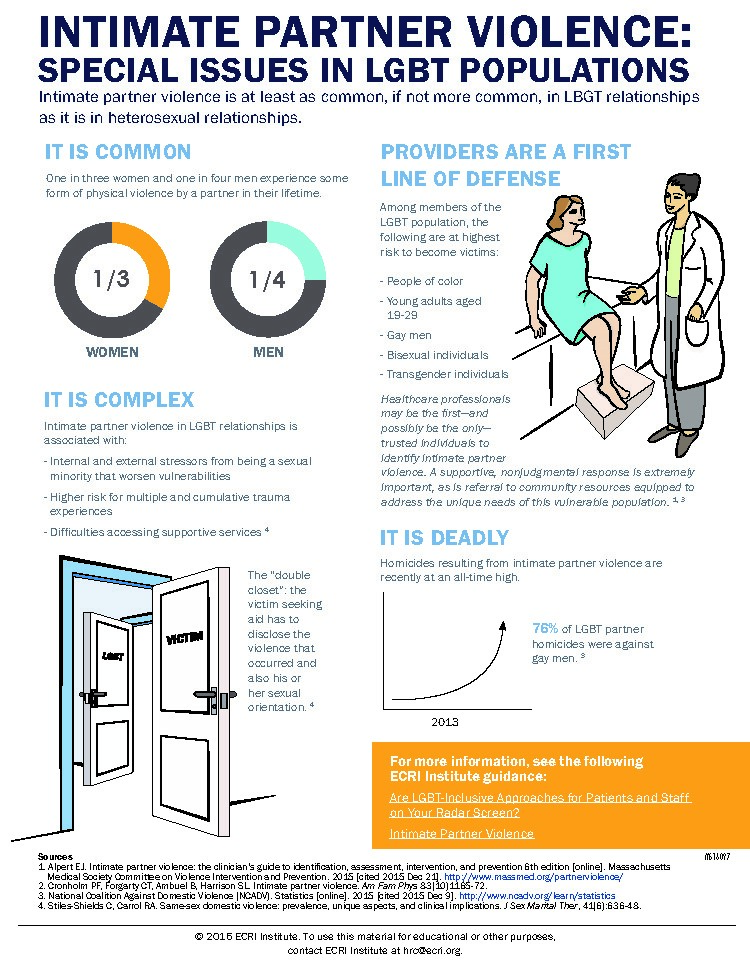
- Provide guidance on LGBT-specific health issues. Numerous resources are available for this purpose. GLMA has developed four separate fact sheets, one each for lesbians, gay men, bisexual individuals, and transgender individuals, identifying the top 10 issues that patients in each group should discuss with their healthcare providers (see Resource List). ECRI Institute has developed a tool for providers addressing the special issues faced by LGBT individuals who experience intimate partner violence (Figure 1).
- Avoid social assumptions. Providers may make assumptions about a person’s sexual orientation or gender identity that affect how they engage with that individual, such as assuming that an older man has a wife who is caring for him. These assumptions can make an LGBT patient uncomfortable even if no harm is intended. A patient who has a masculine or feminine appearance or name may have a different birth gender than the gender the patient identifies, and a patient wearing a wedding band may have a same-sex spouse.
- Avoid assumptions that could erroneously influence clinical decisions. For example, a sexually active individual who presents as male but has female reproductive organs could be pregnant and require appropriate precautions for certain procedures and medications. Similarly, office staff must be prepared for transgender male patients who request mammograms and Pap screening tests and for transgender female patients who require prostate exams.
Providers and organisations can take the following steps to create a welcoming environment for LGBT patients and families:
- Display HEI leadership designation and other indicators of inclusion (e.g., the rainbow flag, a pink triangle, and/or a safe zone sign) on placards, staff badges, and the organisation’s website alongside its patient nondiscrimination and visitation policies.
- Identify LGBT-welcoming providers at the organisation through a website or directory. GLMA also maintains a provider directory for listing LGBT-welcoming physicians and other healthcare professionals at no charge.
- Ensure that the organisation’s website and materials in waiting rooms and other surroundings visually reflect LGBT patients and families.
- Provide the option of gender-neutral restrooms, which can also serve parents and caregivers assisting other-sex children and individuals with disabilities.
- Develop rooming policies proactively rather than waiting until a transgender patient is admitted. Lambda Legal provides guidance on transgender-affirming hospital policies, such as room assignments and protocols for interacting with transgender patients (see Resource List).
- Ask about a patient’s preferred name and pronoun. A transgender patient’s legal name in hospital records may be different from the patient’s preferred name if the patient has not changed their legal identity documents, but people who are transgender will have a better experience when they are called by their preferred name and gender. Hospitals might consider the approach used by Cincinnati Children’s Hospital: It included a flag in patients’ electronic medical records to specify how each patient prefers to be addressed, as well as to provide other pertinent information.
- Design inclusive forms. Admission, registration, and other forms should provide inclusive options that allow LGBT patients to voluntarily self-report sexual orientation and gender identity, as The Joint Commission recommends in its field guide. The forms should provide options to identify a relationship status other than husband or wife and to ask about a child’s parents or guardians in a way that is inclusive of same-sex parents.
Looking ahead
Given the dynamic and multifaceted nature of the driving forces behind LGBT inclusion, implementation of best practices for care delivery will continue to be a moving target across the continuum of care for some time. For example, medical schools, which devote a median of five curriculum hours to LGBT-related issues, have been called upon to better address the needs of LGBT patients (Hollenback, Eckstrand, & Dreger, 2014) and students (Snowdon, 2013). Beginning in 2017, achieving HEI leadership designation will require many additional best practices aside from the original four criteria (Human Rights Campaign Foundation, 2016). Long-term care facilities can also expect increased scrutiny of their practices for LGBT equality (LGBT MAP/SAGE, 2010). Providers and organisations may want to familiarise themselves with the following resources to support ongoing efforts toward inclusion.
Jennifer Comerford is a risk management analyst at ECRI Institute in Plymouth Meeting, Pennsylvania. She can be reached at jcomerford@ecri.org.
Cynthia Wallace is a senior risk management analyst at ECRI Institute in Plymouth Meeting, Pennsylvania. She can be reached at cwallace@ecri.org.
References
Baldhas, T. (2015, February 19). Pediatrician wouldn’t treat baby with 2 moms [online]. Detroit Free Press.Retrieved from http://www.freep.com/story/news/local/michigan/macomb/2015/02/18/discrimination-birth/23640315
Daniel, H., & Butkus, R. (2015). Lesbian, gay, bisexual, and transgender health disparities: Executive summary of a policy position from the American College of Physicians. Annals of Internal Medicine, 163, 135–137. doi:10.7326/M14-2482
Dunne, N. (2014, September 18). Domestic violence likely more frequent for same-sex couples. Northwestern University. Retrieved from http://www.northwestern.edu/newscenter/stories/2014/09/domestic-violence-likely-more-frequent-for-same-sex-couples.html
ECRI Institute. (2015, September 21). Are LGBT-inclusive approaches for patients and staff on your radar screen?Plymouth Meeting, PA: Author.
Gates, G. J. (2011 April). How many people are lesbian, gay, bisexual, and transgender? Los Angeles, CA: Williams Institute. Retrieved from http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf
Health Resources and Services Administration. (n.d.). LGBT health. Retrieved March 28, 2016, from http://www.hrsa.gov/lgbt/
Hollenbach, A. D., Eckstrand, K. L., & Dreger, A. (2014). Implementing curricular and institutional climate changes to improve health care for individuals who are LGBT, gender nonconforming, or born with DSD: A resource for medical educators. Washington, DC: Association of American Medical Colleges. Retrieved from https://www.aamc.org/download/414172/data/lgbt.pdf
Human Rights Campaign Foundation. (2016). Healthcare equality index 2016: Promoting equitable and inclusive care for lesbian, gay, bisexual and transgender patients and their families. Retrieved from http://hrc-assets.s3-website-us-east-1.amazonaws.com//files/assets/resources/HEI_2016_FINAL.pdf
The Joint Commission. (2011). Advancing effective communication, cultural competence, and patient- and family-centered care for the lesbian, gay, bisexual, and transgender (LGBT) community: A field guide. Retrieved March 30, 2016, from http://www.jointcommission.org/lgbt
Lambda Legal. (2010). When health care isn’t caring: Lambda Legal’s survey of discrimination against LGBT people and people with HIV. Retrieved from http://www.lambdalegal.org/sites/default/files/publications/downloads/whcic-report_when-health-care-isnt-caring.pdf
LGBT Movement Advancement Project (MAP) & Services and Advocacy for Gay, Lesbian, Bisexual and Transgender Elders (SAGE). (2010). Improving the lives of LGBT older adults. Retrieved from https://www.lgbtagingcenter.org/resources/pdfs/ImprovingtheLivesofLGBTOlderAdultsLargePrint.pdf
Magdali, K. (2015, July 16). LGBT discrimination in health care: Heterosexual providers found to hold bias on sexual orientation. Medical Daily. Retrieved from http://www.medicaldaily.com/lgbt-discrimination-health-care-heterosexual-providers-found-hold-bias-sexual-343436
Marzuli, J. (2016, February 16). Gay man sues Brooklyn hospital for discrimination, claims he was ignored and ridiculed by homophobic employees. Daily News. Retrieved from http://www.nydailynews.com/new-york/brooklyn/gay-man-sues-brooklyn-methodist-hospital-discrimination-article-1.2520737
Nondiscrimination in health programs and activities. Final rule. (May 18, 2016). Retrieved from https://www.federalregister.gov/articles/2016/05/18/2016-11458/nondiscrimination-in-health-programs-and-activities
Rumble v. Fairview Health Servs., No. 14-CV-2037 (D. Minn. Mar. 16, 2015).
Sabin, J. A., Riskind, R. G., & Nosek, B. A. (2015). Health care providers’ implicit and explicit attitudes toward lesbian women and gay men. Am Journal of Public Health, 105(9), 1831–1841. doi:10.2105/AJPH.2015.302631
Snowdon, S. (2013). Recommendations for enhancing the climate for LGBT students and employees in health professional schools: A GLMA white paper. Retrieved from http://www.glma.org/_data/n_0001/resources/live/Recommendations%20for%20Enhancing%20LGBT%20Climate%20in%20Health%20Professional%20Schools.pdf
Trull, A. (2015, June 22). Can MedStar Georgetown deny breast implant surgery to transgender woman? WAMU 88.5. Retrieved from http://wamu.org/news/15/06/22/is_medstar_georgetown_discriminating_by_refusing_to_do_breast_implant_surgery_for_transgender_woman